What is the dead space in lungs
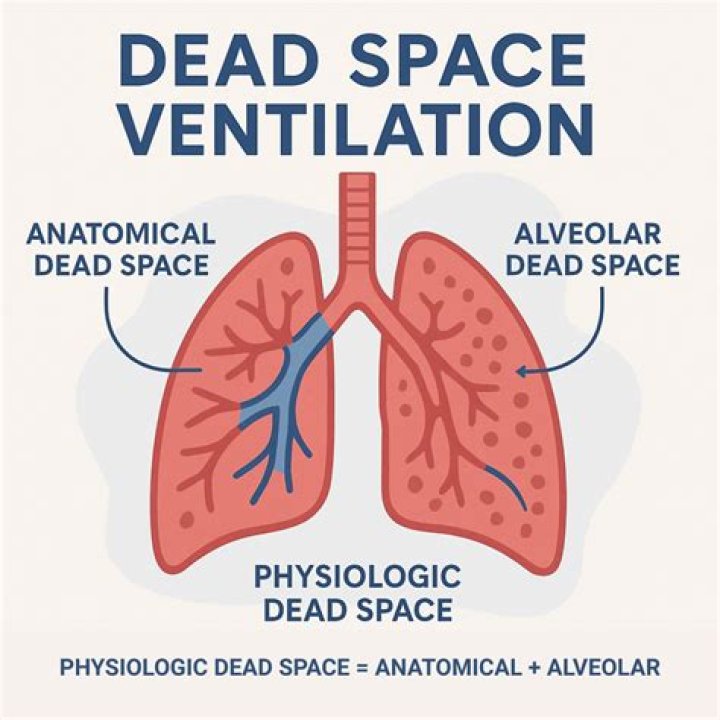
Dead space represents the volume of ventilated air that does not participate in gas exchange. … One can see an increase in the value of physiologic dead space in lung disease states where the diffusion membrane of alveoli does not function properly or when there are ventilation/perfusion mismatch defects.
What causes dead space in lungs?
The alveolar deadspace is caused by ventilation/perfusion inequalities at the alveolar level. The commonest causes of increased alveolar deadspace are airways disease–smoking, bronchitis, emphysema, and asthma. Other causes include pulmonary embolism, pulmonary hypotension, and ARDS.
What is anatomical dead space in the lungs?
The anatomic dead space is the gas volume contained within the conducting airways. The normal value is in the range of 130 to 180 mL and depends on the size and posture of the subject.
What is the respiratory dead space?
Dead space is the volume of air that is inhaled that does not take part in the gas exchange, because it either remains in the conducting airways or reaches alveoli that are not perfused or poorly perfused. It means that not all the air in each breath is available for the exchange of oxygen and carbon dioxide.What are the types of dead space?
There are three different types of dead space; anatomic, alveolar, and equipment/mechanical. Dead space ventilation involves that component of the respiratory gases that does not participate in gas exchange.
What happens when dead space is increased?
At a fundamental level, increasing the dead space functionally indistinguishable from hypoventilation: Dead space is a fraction of the total tidal volume. Of the tidal volume, only the non-dead fraction participates in gas exchange. Ergo, increasing dead space has the same effect as reducing the tidal volume.
What is significance of dead space?
Dead space has particular significance in the concept of ventilation (V) and perfusion (Q) in the lung, represented by the V/Q ratio. Alveoli with no perfusion have a V/Q of infinity (Q=0), whereas alveoli with no ventilation have a V/Q of 0 (V=0).
What is the difference between dead space and shunt?
The main difference between the shunt and dead space is that shunt is the pathological condition in which the alveoli are perfused but not ventilated, whereas dead space is the physiological condition in which the alveoli are ventilated but not perfused.How do you measure dead space?
The “anatomical” dead space is commonly measured by sampling an inert gas (N2) and volume in the exhalation following a large breath of oxygen (VD(F)). It may also be measured from an inert gas washout (VD(O)) that describes both volume and the delivery of VD(O) throughout the expiration.
What is the difference between psychological dead space and anatomical dead space?Anatomical dead space is the air-filled in conducting airways and does not participate in gas exchange. Meanwhile, physiological dead space is the sum of all parts of the tidal volume that does not participate in gas exchange.
Article first time published onWhat is the relationship between anatomical and alveolar dead space?
Alveolar dead space is the volume of gas which fills lung units which are underperfused / not perfused / not participating in gas exchange (pick the description which produces the fewest furrows in the examiner’s brow) It is the difference between physiological dead space and anatomical dead space.
Does asthma increase dead space?
The effect of airways obstruction on the dead space volumes was studied in 36 children with asthma and 28 with cystic fibrosis. Physiological dead space increased with increasing airways obstruction.
Can dead space cause hypoxemia?
If underlying pathophysiology causes a problem with ventilation and/or perfusion in the form of a shunt or dead space, the resultant VQ mismatch will cause hypoxemia.
Why does dead space increase with age?
The lung parenchyma loses its supporting structure causing dilation of air spaces: “senile emphysema”. … The alveolar dead space increases with age, affecting arterial oxygen without impairing the carbon dioxide elimination.
Does COPD cause dead space?
In advanced COPD, physiological dead space (wasted ventilation) is increased as a consequence of underlying V/Q mismatch. As a result, patients with COPD must adopt a higher minute ventilation in order to keep alveolar ventilation (and hence Paco2) constant.
How do you lower dead space?
Adjustments in ventilation rates and the use of positive end-expiratory pressure (PEEP) are used to decrease dead space. Although multiple studies have failed to show this expected effect consistently, it is still widely used in cases of ARDS.
What happens to dead space during exercise?
Figure 6. Dead space ventilation at differing levels of work. During exercise, dead space ventilation falls with increasing work, owing to increasing Vts. In the high–dead space group, dead space ventilation is significantly higher throughout exercise, and this difference is exaggerated with increasing work.
Where is anatomic dead space?
Anatomic dead space specifically refers to the volume of air located in the respiratory tract segments that are responsible for conducting air to the alveoli and respiratory bronchioles but do not take part in the process of gas exchange itself.
How does tracheostomy reduce dead space?
Proponents of early tracheostomy argue that decreases in anatomic dead space lower airway resistance, allow lower peak inspiratory pressures and may even change dynamic compliance, resulting in reduction of the work of breathing, thus allowing patients to wean off the ventilator expeditiously and decrease ventilator …
Is pneumonia shunt or dead space?
A pulmonary shunt often occurs when the alveoli fill with fluid, causing parts of the lung to be unventilated although they are still perfused. Intrapulmonary shunting is the main cause of hypoxemia (inadequate blood oxygen) in pulmonary edema and conditions such as pneumonia in which the lungs become consolidated.
Does dead space improve with oxygen?
Dead spaces can severely impact breathing, because they reduce the surface area available for gas diffusion. As a result, the amount of oxygen in the blood decreases, whereas the carbon dioxide level increases.
Is ARDS shunt or dead space?
Acute respiratory distress syndrome (ARDS) is characterized by severe impairment of gas exchange. Hypoxemia is mainly due to intrapulmonary shunt, whereas increased alveolar dead space explains the alteration of CO2 clearance.
How does peep increase dead space?
It is accepted that positive-pressure ventilation with PEEP increases Bohr dead space by dilating the conducting airways and decreasing pulmonary capillary perfusion at the alveolar level. Thus, dead space is considered a surrogate of lung stress despite lack of clear evidence.
What is alveolar ventilation equal to?
Although alveolar ventilation is usually defined as the volume of fresh air entering the alveoli per minute, a similar volume of alveolar air leaving the body per minute is implicit in this definition.
What is the normal minute ventilation?
Normal minute ventilation is between 5 and 8 L per minute (Lpm). Tidal volumes of 500 to 600 mL at 12–14 breaths per minute yield minute ventilations between 6.0 and 8.4 L, for example. Minute ventilation can double with light exercise, and it can exceed 40 Lpm with heavy exercise.
What are the 5 causes of hypoxia?
Hypoxemia is caused by five categories of etiologies: hypoventilation, ventilation/perfusion mismatch, right-to-left shunt, diffusion impairment, and low PO2.
What are the symptoms of hypoxia?
- Headache.
- Shortness of breath.
- Fast heartbeat.
- Coughing.
- Wheezing.
- Confusion.
- Bluish color in skin, fingernails, and lips.